Brachial Plexus Injury
The brachial plexus is a group of separate nerves that begin in a tiny area of the body where cervical nerves 5, 6, 7, 8 and thoracic nerve 1 exit the spinal cord. It ends just above the clavicle or collar bone. There are two brachial plexuses, one on each side of the body. Each brachial plexus is organized in an extremely small space and in a complicated pattern. These nerves branch out of the spinal cord in the neck (cervical spine), follow the same pathway at the top of the shoulder, collect under the clavicle (collar bone) and eventually divide as they travel down the arms. They branch into specific nerves which provide distinct functions in the arm, hand, and fingers. Together, they look like a bunch of nerves tossed together, but they actually follow a very specific pattern.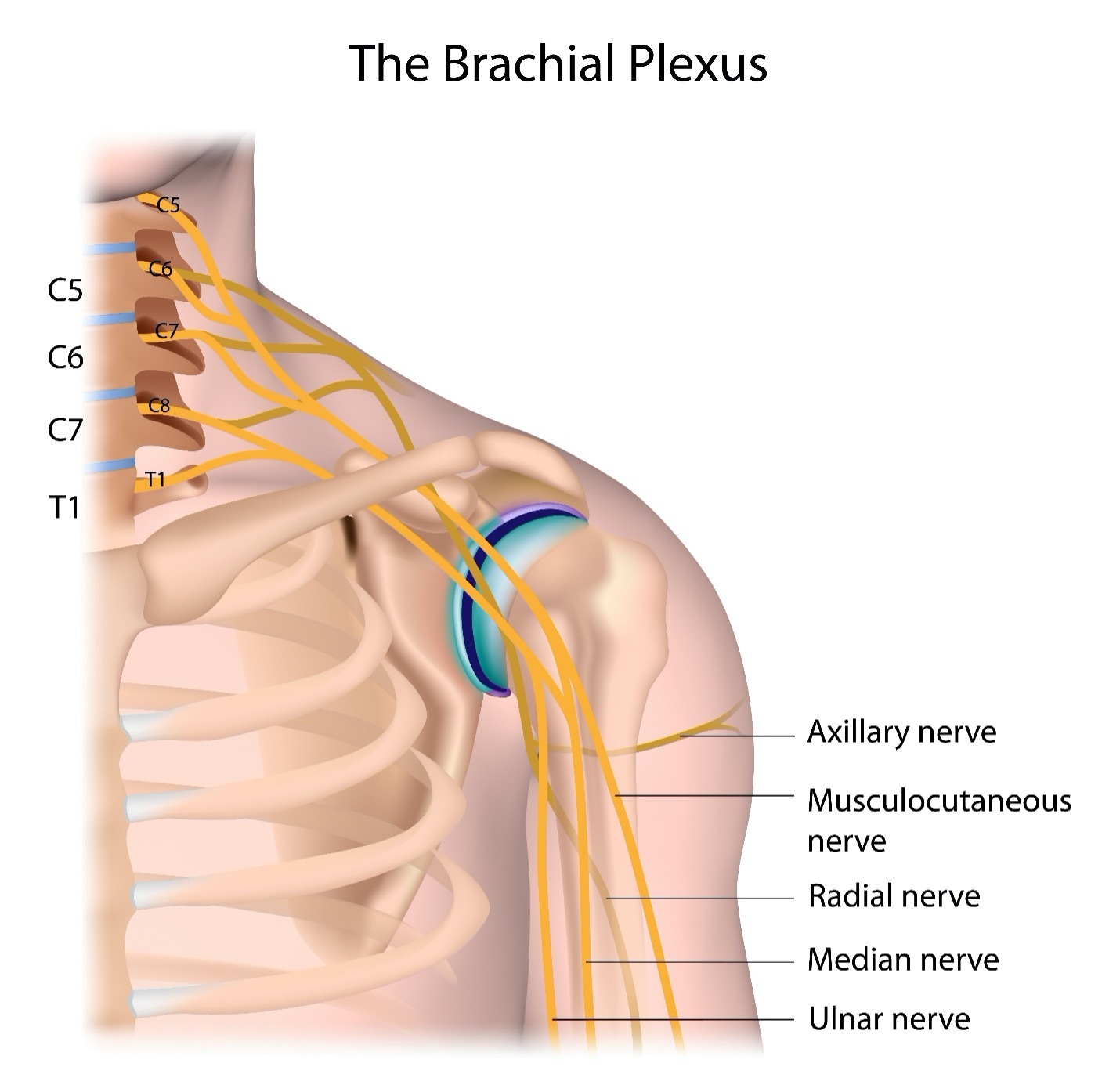
Nerve Pattern of the Brachial Plexus
To create the brachial plexus, nerves exit from C5-8 and T1 levels of the spinal cord. The spinal nerves spilt combining with other branches to make the brachial (arm) plexus (network of nerves). The nerves connect in a specific pattern. The nerve roots that exit highest in the spinal cord at C5 and C6 basically join to create the musculocutaneous nerve. The nerve root that exits C7 becomes the axillary, median and radial nerves. The nerve roots at C8 and T1 join to form the ulnar nerve. However, notice in the diagram there is a variety of cross functions of nerves within the brachial plexus. Multiple branches of nerves extend from each of the main spinal nerves. This is what makes the brachial plexus such a complicated formation of nerves and thereby resulting function. Imagine all these cross connections in an extremely small space that is close to the skin making it very vulnerable to injury. The following diagram shows the nerve organization of the brachial plexus more clearly.
Nerves of the brachial plexus are like a web of connections with sources of the nerve originating from the spinal cord nerve roots but with added connections and crossovers to other nerve roots within the plexus. The routes of the nerves are outlined in the figure above. If a function is slowed or absent, the brachial plexus nerves injured are within that complicated pathway. These are the functions of the nerves in the brachial plexus:
| Nerve | Action |
|---|---|
| Musculocutaneous | Upper arm muscles flexing, shoulder, and elbow |
| Axillary | Shoulder rotation, arm lifting away from body |
| Median | Forearm and hand movement |
| Radial | Upper arm, elbow, forearm, and hand movement |
| Ulnar | Finger movement |
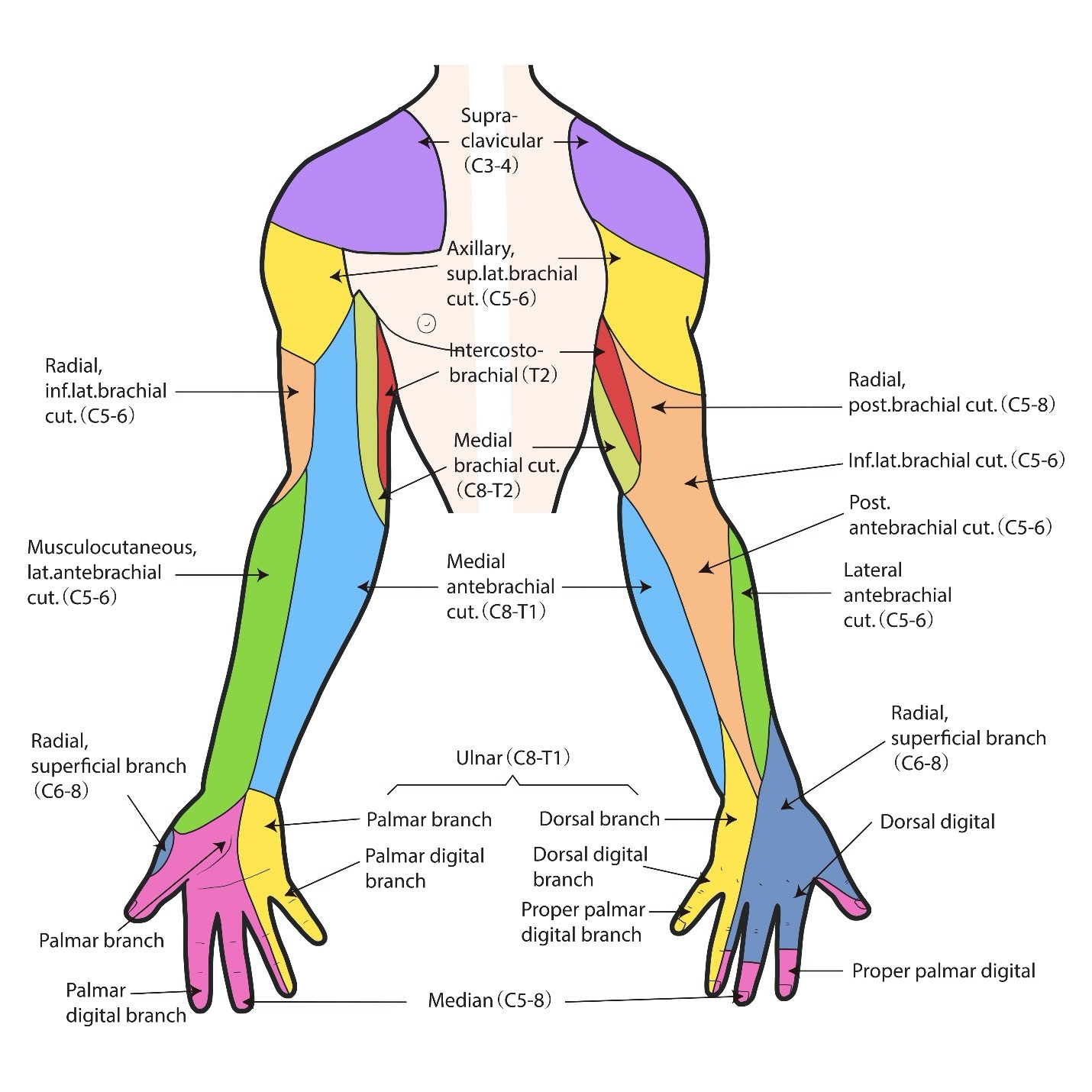
Sensation is also controlled by the nerves that travel through the brachial plexus. Distribution of sensation by spinal nerve root is shown in the following figures. The area of sensation is called a dermatome. If sensation is decreased or diminished, an injury or entrapment of the specific nerve or to the brachial plexus could be the source. Loss of sensation can accompany a brachial plexus injury.
Brachial Plexus Injury
Injury to the brachial plexus can occur in a variety of ways including both trauma and disease. Typically, injury is just on one side of the body, but both brachial plexuses can be injured in rare cases depending on the event. When an injury occurs, function, sensation or both can be affected. The location and extent of the injury determines which nerves lose some or all communication with the spinal cord that transmits messages to and from the brain. Duration of brachial plexus injury can range anywhere between brief or long-lasting.
The peripheral nerves are nerves outside of the brain and spinal cord. An injury that affects the brachial plexus nerves in the shoulder area is a peripheral nerve injury. However, if the brachial plexus injury involves the nerve roots, part of the spinal cord can also be affected. The location of the injury affects the treatment.
Causes of brachial plexus injuries can occur from birth trauma (difficult delivery), blunt trauma (something forcefully hitting against the neck or upper shoulder, stretching, or compressing the nerves), athletics (in any sport but often seen on the football field and in gymnastics or cheerleading), gunshot wounds, motor vehicle accidents, medical trauma, cancer, and radiation therapy.
What happens to the nerves in the brachial plexus can be from these types of injuries:
Overstretching The nerves are stretched too far (neuropraxia). Nerves have a bit of stretching ability to accommodate movement in the body. Overstretched nerves are not severed or bumped but pulled past their ability to accommodate extreme movement. Much like elastic that is stretched too far, they do not snap back. This can be from compression on the nerve root when something in the vertebral bones does not allow the natural stretch of the nerve to occur such as arthritis or from traction of the nerves in an injury when the nerve is pulled downward past its natural elasticity. This injury typically produces a burning, stinging, or electrical shock pain in the arm.
Birth A very small number of infants have brachial plexus at the time of birth. This can occur from a variety of issues. Shoulder dystocia is diagnosed if the neck and shoulder of the baby is overstretched at the time of delivery. A large baby, small birth canal, breach birth, use of forceps or other birth device assistance, difficulty breathing, and diabetes are risk factors associated with brachial plexus birth injury. Many infants with these same risk factors do not have brachial plexus injury.
Rupture of the brachial plexus nerve occurs when overstretching goes so far that the nerve is actually pulled apart. This can include an entire nerve separation, fibers within a nerve being torn, or the injury occurring to the myelin sheath (the fatty substance that protects nerve transmissions). This injury creates severe pain. The damaged nerve cannot transmit messages leaving their target muscles unstable and weak. Surgery is required to repair the nerve or nerves.
Compression injuries are from an outside force pinching nerves within the brachial plexus or from internal injury. This stops the ability for nerves to transmit messages.
Scar Tissue Just as skin creates a scar when it heals, so do other parts of your internal body. This is a natural process. Scar tissue of a nerve can prevent messages from transmitting. It also creates pain. Scar tissue may need to be surgically removed followed by the affected nerve being grafted to another nerve or ‘capped’ to avoid the scar from reforming.
Avulsion is a complete detachment of one or more nerves in the brachial plexus at the nerve root. Reattachment creates issues because the location of the injury is at the nerve root that attaches directly to the spinal cord which is in the central nervous system (CNS). It is extremely painful and typically accompanied with other soft tissue and bone fractures. This occurs from extreme traumatic injury. Results are weakness, paralysis, and loss of sensation in the areas served by the avulsed nerve or nerves.
Tumor and Radiation can also be causes of brachial plexus injury. Tumors (neuromas) can be on a nerve or nerves of the brachial plexus or near the brachial plexus pushing on it. They can distort the pathway or pull the nerve overstretching them from within the body. If radiation is used for tumor treatment, to the chest or shoulder area, damage to the nerves can possibly occur.
Symptoms of Brachial Plexus Injury
Since brachial plexus injuries are typically on one side of the body, symptoms will be felt in the shoulder, hand, or arm on that same side. Symptoms include numbness, loss of feeling, loss of movement, burning, stinging, tingling, shooting pain, stiff joints, and muscle atrophy (wasting). The arm may have some or no function, some, or no sensation. The hand is most often turned inward. The arm may be smaller and shorter.
Symptoms of brachial plexus injury are the same as with any nerve injury. Most individuals know what it is like to ‘hit your funny bone’ in the elbow. This is really an uneventful tap to the nerve close to the surface of the skin in the elbow. The pain is mild and temporary. Some have felt nerve pain in a sore tooth. Because the brachial plexus consists of nerves, the pain associated with injury can be extreme.
Symptoms of brachial plexus injury depend on the location and significance of the injury. They may be temporary in a mild injury or severe in more involved injuries. They can appear slowly or suddenly. Duration of the symptoms may last a short (hours, days, weeks) to long (years) time. Symptoms can be intermittent such as only when you turn your head a certain way or move your shoulder, arm, or hand. Brachial plexus injury can be severe and quite debilitating. Results of brachial plexus injury appear in the area that the injured nerve serves. The Nerve/Action table and Arm Dermatomes figure above can help you understand where your brachial plexus injury is located.
Brachial Plexus Syndromes and Palsies
Some brachial plexus injuries result in a particular pattern. These are classified by syndrome or palsy.
Brachial neuritis (nerve inflammation) also known as Parsonage Turner syndrome occurs with a sudden onset of severe shoulder and upper arm pain. It progresses to weakness, muscle loss and loss of sensation. It usually is due to an unknown source but thought to be related to an autoimmune response from infection, injury, or childbirth. This neuritis can also appear in other peripheral nerves specifically the diaphragm and legs.
Erb’s palsy results from an injury to the upper brachial plexus typically on one side of the body affecting the shoulder and elbow. It leads to numbness, and reduced shoulder and elbow function. Lifting the arm or bringing the hand toward the body is restricted. Erb’s palsy can occur at any time but is the most common brachial plexus classification injury at birth. A mild Erb’s palsy can be treated with therapy while severe cases may require surgery.
Klumpke’s palsy is an injury to the lower part of the brachial plexus at birth on one side of the body. There is loss of movement, sensation, or both at the wrist and hand resulting in loss of finger function. A mild Klumpke’s palsy can be treated with therapy while severe cases may require surgery.
Horner Syndrome is a specific issue in some individuals with brachial plexus injury. Symptoms include a droopy eyelid, constricted pupil, and decreased facial sweating on the side of the brachial plexus injury. It is caused from injury to the nerves in the sympathetic nervous system, the part of the autonomic nervous system (ANS) that slows body functions.
Diaphragm paralysis or palsy has been noted in rare cases. The long thoracic nerve is located near the spinal nerve roots in the brachial plexus area which contributes to function of the diaphragm. Because the injury to the brachial plexus can extend to surrounding tissue, functions of the long thoracic nerve can also be affected.
Diagnosing Brachial Plexus Injury
To determine if an injury to the brachial plexus is present, your primary healthcare provider, neurologist, or nerve specialist will perform a neurological examination with particular detail in assessment of the affected area of the neck, shoulder, chest, arm, hands and fingers or from C4 to T3/4. This range includes an area a bit wider than what is served by the nerves of the brachial plexus to assess for collateral injury.
Sensory ability is assessed at each dermatome (body area controlled by each nerve). Assessments include light (cotton swab) and sharp (pin prick) touch, temperature testing warmth and coolness, and proprioception (sensing where a body part is in space).
Movement is also assessed. This includes level of gross and fine motor function, presence of tone (spasticity), range of motion, individual muscle power, and deep tendon reflexes.
Coordination is then evaluated. Typical assessments are the finger to nose, and rapid alternating movement in the arm, hands, and fingers.
Imaging studies will include X-ray, MRI, CT scan and/or ultrasound to view the detailed specifics of the brachial plexus and surrounding tissues and blood vessels.
Electrodiagnostic studies include electromyogram (EMG) which assesses muscle function. Nerve conduction studies (NCS) assess how well the nerve transmits messages.
An angiogram may be done to check blood flow to the area. This is performed by injecting dye into the blood vessels to look for injury, broken vessels, or clots.
Treatment for Brachial Plexus Injury
Level of treatment depends on the severity of injury. Brachial plexus injuries from mildly overstretched nerves are often treated conservatively. Injuries where the nerve is torn especially with rupture, neuroma (tumor), and avulsion requires surgery. Severely overstretched brachial plexus injuries can also require surgical intervention.
Conservative treatments include:
- Physical therapy for arm mobility and strength, electrical stimulation, muscle stretches, range of motion and balance.
- Occupational therapy to learn techniques for activities of daily living and to obtain devices to improve independence such as use of button hooks and zipper pulls.
- Medications may be used such as steroid creams or injections to reduce inflammation and for pain control.
- Shoulder supports, splints, and/or compression garments may be used to support the limb, increase function without further injury to the nerve(s) and to control pain.
- Electrical stimulation may be gently supplied by electrodes placed on the skin to stimulate healing and control pain.
Surgical intervention, if needed, should be performed within six months of injury for adults. For infants with brachial plexus injury occurring at birth, surgery is at four to six months. Previously six months was the wait time to see if any return occurred, however, current research indicates surgery should be within the first six months from injury for best outcomes.
Surgical options may include some or all the following procedures. Surgeries include reconnecting nerves, removing scar tissue (neurolysis), nerve grafts from a functioning nerve to an affected nerve, nerve transfers which is moving a redundant nerve to improve function, placement of an internal nerve stimulation device, and transferring tendons and muscles to improve function. More than one surgery may be required for best results.
Surgery of the nerve should be performed by an individual with extensive education in the procedure. There is typically a recovery time where the arm is not used to allow the internal surgical site to heal. Then therapy begins to learn to use the new functions of your shoulder, arm, hands, or fingers.
Treatments may be provided for issues with extreme nerve pain that cannot be controlled with medication, or surface procedures such as electrical stimulation or nerve block stimulators. Injections may assist with pain control or surgical procedures and implants to block pain signal transmissions.
Recovery from brachial plexus injury may take from weeks to months or even years. Continued therapy to avoid complications and to enhance progression must be maintained. Assessments of progress will be completed every other week to every month.
It is important to note that nerves in the body regenerate at a rate of approximately one inch per month. Issues that affect healing include ongoing injury from infection or disease, lack of treatment or nerve shock. Once an injury is sustained, the nerve might be in shock for a period of time, but it will begin to regenerate.
The Rehabilitation Healthcare Team
Many healthcare providers work together to care for individuals with brachial plexus injury. Individuals who might be involved with your treatment for brachial plexus injury include:
Physiatrist or primary healthcare provider will provide diagnostic and conservative care, monitoring your progress. Physiatrists are physicians that specialize in physical medicine and rehabilitation.
Surgeon If surgery is necessary, you will be referred to a neurosurgeon, orthopedic surgeon, plastic and reconstructive surgeon or hand surgeon depending on the specific needs of your case. This highly educated individual will perform nerve surgery, muscle and/or tendon surgery as needed.
Physical Therapist is an individual who will provide and guide your treatment for gross motor movement such as passive and active movement in conservative treatment and before and after surgery if needed.
Occupational Therapist will provide treatment for fine motor movement as needed. They will assist with adaptations for eating, dressing, bathing, toileting, and work needs.
Research
Much research about prevention of brachial plexus injury is underway. Techniques to avoid brachial plexus injury in the delivery process for infants and prevention techniques for adults to avoid injury due to radiation therapy and accidents is ongoing.
Treatments of brachial plexus injury are evolving. Research of neuromuscular electrical stimulation in complex injuries as well as treatments using conservative therapeutic exercises is under study.
For those who require surgical repair of brachial plexus injury, work focuses on nerve repair, grafting and reimplantation of avulsed nerves into the spinal cord. Discoveries in the timing of brachial plexus repair surgery have improved outcomes. The use of transferring nerves from one human to another while avoiding rejection is making great strides.
Facts and Figures
Brachial plexus injury at birth occurs in 1-2/1000 births. Spontaneous recovery rate is 66%.
Trends in brachial plexus injury is lowering in vaginal births but increasing in cesarean section births.
The number of adult and teen brachial plexus injuries is rising due to motor vehicle accidents and sports-related injury.
In a study by Kaiser, et al. (2020) rate and types of brachial plexus injuries in adults are:
Brachial Plexus Injury rates are closed (no skin opening) 93%, lacerations 3%, gunshot wounds (GSWs) 3%
Cause of closed brachial plexus injuries was motorcycle accidents 67%, car crashes 14%
Complete lesions 53%, upper plexus injury 39%, lower plexus injury 6%
Males outnumber females 9:1
Resources
If you are looking for more information about brachial plexus injury or have a specific question, our Information Specialists are available business weekdays, Monday through Friday, toll-free at 800-539-7309 from 9:00 am to 8:00 pm ET.
Additionally, the Reeve Foundation maintains a fact sheet collection with resources from trusted sources. Check out our repository of fact sheets on hundreds of topics ranging from state resources to secondary complications of paralysis.
We encourage you to also reach out to brachial plexus support groups and organizations for individuals and families, including:
National Institutes of Health website: https://search.nih.gov/search?utf8=%E2%9C%93&affiliate=nih&query=brachial+plexus&commit=Search
United Brachial Plexus Network https://ubpn.org/
References
Al-Qattan MM. The outcome of Erb’s palsy when the decision to operate is made at 4 months of age. Plast Reconstr Surg. 2000 Dec;106(7):1461-5. doi: 10.1097/00006534-200012000-00003. PMID: 11129172.
Bain JR, Dematteo C, Gjertsen D, Hollenberg RD. Navigating the gray zone: a guideline for surgical decision making in obstetrical brachial plexus injuries. J Neurosurg Pediatr. 2009 Mar;3(3):173-80. doi: 10.3171/2008.12.PEDS0885. PMID: 19338462.
Benjamin K. Part 2. Distinguishing physical characteristics and management of brachial plexus injuries. Adv Neonatal Care. 2005 Oct;5(5):240-51. doi: 10.1016/j.adnc.2005.06.001. PMID: 16202966.
Caillaud M, Richard L, Vallat JM, Desmoulière A, Billet F. Peripheral nerve regeneration and intraneural revascularization. Neural Regen Res. 2019 Jan;14(1):24-33. doi: 10.4103/1673-5374.243699. PMID: 30531065; PMCID: PMC6263011.
Cattin AL, Lloyd AC. The multicellular complexity of peripheral nerve regeneration. Curr Opin Neurobiol. 2016 Aug;39:38-46. doi: 10.1016/j.conb.2016.04.005. Epub 2016 Apr 26. PMID: 27128880.
Coroneos CJ, Voineskos SH, Christakis MK, Thoma A, Bain JR, Brouwers MC; Canadian OBPI Working Group. Obstetrical brachial plexus injury (OBPI): Canada’s national clinical practice guideline. BMJ Open. 2017 Jan 27;7(1):e014141. doi: 10.1136/bmjopen-2016-014141. PMID: 28132014; PMCID: PMC5278272.
Griffith JF. Ultrasound of the brachial plexus. Semin Musculoskelet Radiol. 2018 Jul;22(3):323-333. doi: 10.1055/s-0038-1645862. Epub 2018 May 23. PMID: 29791960.
Kaiser R, Waldauf P, Ullas G, Krajcová A. Epidemiology, etiology, and types of severe adult brachial plexus injuries requiring surgical repair: systematic review and meta-analysis. Neurosurg Rev. 2020 Apr;43(2):443-452. doi: 10.1007/s10143-018-1009-2. Epub 2018 Jul 17. PMID: 30014280.
Limthongthang R, Bachoura A, Songcharoen P, Osterman AL. Adult brachial plexus injury: evaluation and management. Orthop Clin North Am. 2013 Oct;44(4):591-603. doi: 10.1016/j.ocl.2013.06.011. Epub 2013 Sep 6. PMID: 24095074.
Lovaglio AC, Socolovsky M, Di Masi G, Bonilla G. Treatment of neuropathic pain after peripheral nerve and brachial plexus traumatic injury. Neurol India. 2019 Jan-Feb;67(Supplement):S32-S37. doi: 10.4103/0028-3886.250699. PMID: 30688230.
Mukherji SK, Castillo M, Wagle AG. The brachial plexus. Semin Ultrasound CT MR. 1996 Dec;17(6):519-38. doi: 10.1016/s0887-2171(96)90002-5. PMID: 9023866.
Noland SS, Bishop AT, Spinner RJ, Shin AY. Adult traumatic brachial plexus injuries. J Am Acad Orthop Surg. 2019 Oct 1;27(19):705-716. doi: 10.5435/JAAOS-D-18-00433. PMID: 30707114.
Oliveira KMC, Pindur L, Han Z, Bhavsar MB, Barker JH, Leppik L. Time course of traumatic neuroma development. PLoS One. 2018 Jul 16;13(7):e0200548. doi: 10.1371/journal.pone.0200548. PMID: 30011306; PMCID: PMC6047790.
Orebaugh SL, Williams BA. Brachial plexus anatomy: normal and variant. ScientificWorldJournal. 2009 Apr 28;9:300-12. doi: 10.1100/tsw.2009.39. PMID: 19412559; PMCID: PMC5823154.
Pirela-Cruz M, Mujadzić M, Kanlić E. Brachial plexus treatment. Bosn J Basic Med Sci. 2005 Aug;5(3):7-15. doi: 10.17305/bjbms.2005.3264. PMID: 16351575; PMCID: PMC7202152.
Pondaag W, Malessy MJA. Evidence that nerve surgery improves functional outcome for obstetric brachial plexus injury. J Hand Surg Eur Vol. 2021 Mar;46(3):229-236. doi: 10.1177/1753193420934676. Epub 2020 Jun 26. PMID: 32588706; PMCID: PMC7897782.
Romaña MC, Rogier A. Obstetrical brachial plexus palsy. Handb Clin Neurol. 2013;112:921-8. doi: 10.1016/B978-0-444-52910-7.00014-3. PMID: 23622302.
Quick TJ, Brown H. Evaluation of functional outcomes after brachial plexus injury. J Hand Surg Eur Vol. 2020 Jan;45(1):28-33. doi: 10.1177/1753193419879645. Epub 2019 Oct 9. PMID: 31597518.
Zhong LY, Wang AP, Hong L, Chen SH, Wang XQ, Lv YC, Peng TH. Microanatomy of the brachial plexus roots and its clinical significance. Surg Radiol Anat. 2017 Jun;39(6):601-610. doi: 10.1007/s00276-016-1784-9. Epub 2016 Nov 19. PMID: 27866248.
